INDEX 01 / RESEARCH RECORD
The CJC-1295 Research Record
Mechanism, pharmacokinetics, the two Phase 1 studies, the terminated Phase 2 trial, and the ipamorelin comparison — read from the published literature.
Fig. 01 / GHRH (1-29) substitutions & DAC linker
Schematic of the GHRH 1-29 backbone with positions 2, 8, 15, and 27 carrying the canonical CJC-1295 substitutions, and the DAC maleimidopropionic-acid linker rendered separately.
CJC-1295 Mechanism of Action
CJC-1295 Mechanism of Action
CJC-1295 is a long-acting GHRH receptor agonist. It binds GHRH receptors on anterior pituitary somatotrophs, activates Gs-protein / adenylyl cyclase / cAMP / PKA signaling, drives CREB phosphorylation and GH gene transcription, and triggers pulsatile GH release into systemic circulation [1]. The released GH then activates hepatic GH receptors via JAK2-STAT5 signaling, raising IGF-1 [3].
The four amino-acid substitutions — D-Ala2, Gln8, Ala15, Leu27 — confer proteolytic stability to the GHRH 1-29 backbone. The D-Ala2 substitution alone substantially increases plasma half-life and reduces metabolic clearance versus unmodified GHRH(1-29) in healthy men [2]. The DAC linker adds a second pharmacokinetic mechanism: a maleimidopropionic-acid moiety on a Lys30 residue forms a covalent thioether bond with Cys34 of circulating serum albumin, producing an approximately 67 kDa peptide-albumin complex that is too large for glomerular filtration and is shielded from proteolytic degradation [1]. The combined effect of the four substitutions and the DAC linker is a plasma half-life of 5.8 to 8.1 days in healthy adults [3].
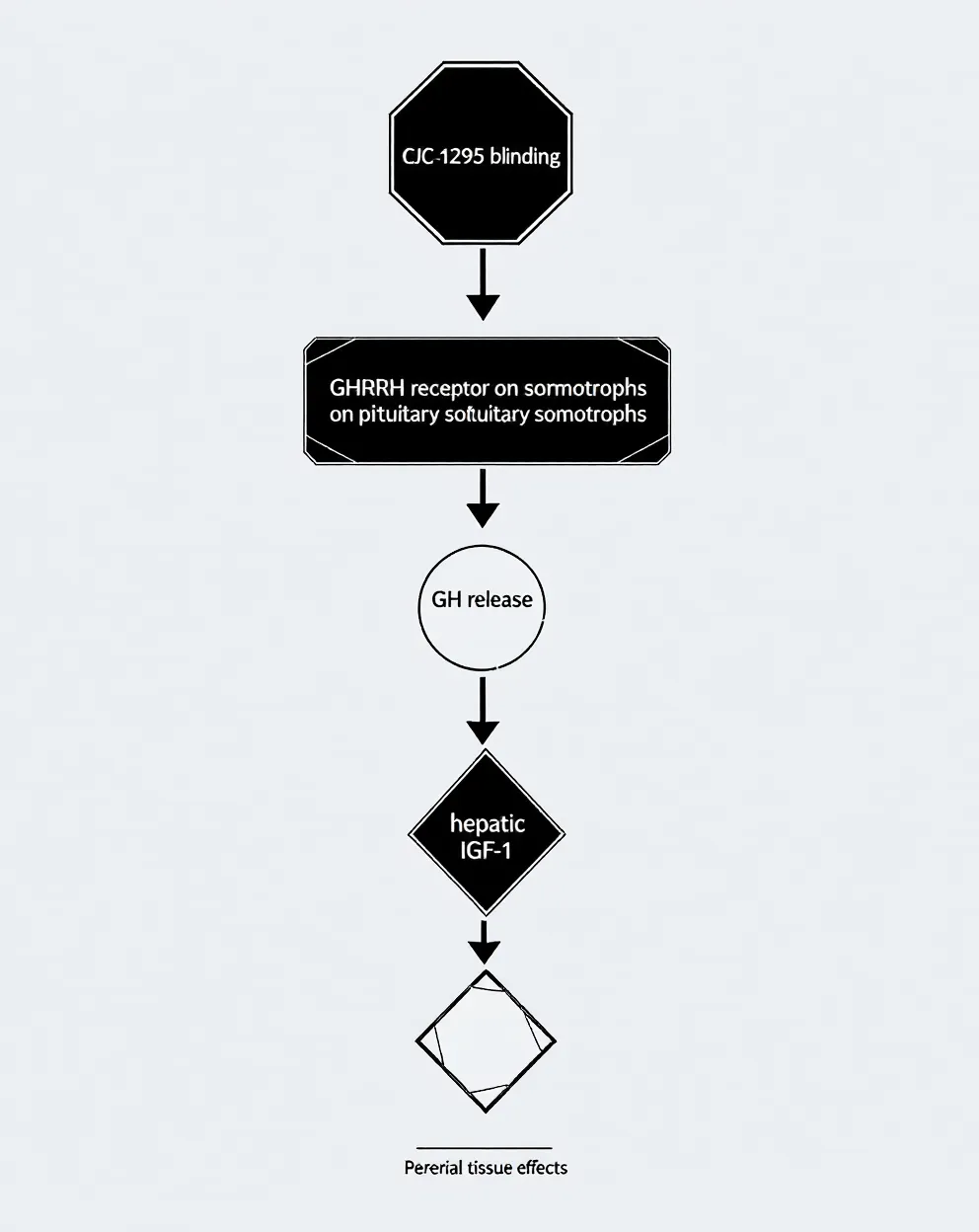
Fig. 02 / GH/IGF-1 signaling cascade
CJC-1295 → GHRH receptor (cobalt-marked) → GH release → hepatic IGF-1 → peripheral tissue effect.
CJC-1295 with DAC vs. without DAC
CJC-1295 with DAC vs. without DAC
The DAC distinction is the dominant structural question in the published record. Both variants share the four amino-acid substitutions to GHRH 1-29. Only the DAC variant carries the maleimidopropionyl-lysine albumin linker.
CJC-1295 with DAC: plasma half-life 5.8-8.1 days in healthy adults (Teichman 2006). Sustained 2-10x GH elevation for six days or more after a single dose; 1.5-3x IGF-1 elevation for nine to eleven days; IGF-1 remained elevated for up to 28 days under weekly or biweekly dosing [3]. The dosing rhythm is once or twice weekly in published Phase 1 and Phase 2 protocols [3][9].
CJC-1295 without DAC (also called modified GRF 1-29): plasma half-life approximately 30 minutes [10]. The pharmacokinetic profile is pulsatile rather than sustained — closer to native GHRH but stabilized against DPP-IV cleavage by the D-Ala2 substitution. Research protocols typically describe the non-DAC variant administered once daily or before bedtime to mimic endogenous GH pulsatility [10].
DAC vs. no-DAC: structural difference
CJC-1295 DAC carries a drug-affinity-complex linker that binds albumin (half-life ~8 days). Without DAC (modified GRF 1-29) the half-life is ~30 minutes, producing a pulsatile rather than sustained GH elevation [1][10]. The pulsatile profile more closely mimics endogenous GHRH; the sustained profile mimics what the DAC platform was engineered to produce.
How does CJC-1295 work?
It acts as a long-acting GHRH agonist. The DAC moiety extends serum half-life from minutes (native GHRH) to roughly 8 days, sustaining pulsatile GH release across the dosing interval (Ionescu 2006 reported preserved pulse frequency and pulse magnitude under continuous CJC-1295 stimulation) [4].
CJC-1295 DAC defined
Drug Affinity Complex variant: a maleimidopropionic-acid linker covalently binds Cys34 of serum albumin after subcutaneous injection, sheltering the peptide from enzymatic degradation and extending half-life to roughly 8 days [1]. The 67 kDa peptide-albumin complex is too large for glomerular filtration.
Modified GRF 1-29 (CJC-1295 without DAC)
The non-DAC version of CJC-1295: the same four amino-acid substitutions to GHRH 1-29, but without the albumin-binding linker [10]. Short half-life (~30 minutes) producing pulsatile GH release. Research protocols typically describe daily or pre-bedtime subcutaneous administration.
Variant.A / With DAC
CJC-1295-DAC
- Half-life5.8–8.1 days
- DosingOnce / twice weekly
- GH patternSustained — 2–10x for 6+ d
- IGF-11.5–3x for 9–11 d
- ReferenceTeichman 2006[3]
Variant.B / No DAC / Modified GRF 1-29
Modified GRF 1-29
- Half-life~30 minutes
- DosingDaily / pre-bedtime
- GH patternPulsatile spike, rapid decay
- IGF-1Transient elevation
- ReferenceModified GRF 1-29 record[10]
Reported Effects in the Literature
Reported Effects in the Literature
What the published clinical studies have actually measured: 2-10x mean plasma GH elevation for six days or more after a single subcutaneous dose of CJC-1295-DAC in healthy adults [3]; 1.5-3x IGF-1 elevation for nine to eleven days [3]; sustained IGF-1 elevation up to 28 days under repeated weekly or biweekly dosing [3]; 7.5-fold trough GH elevation and 46% mean GH increase under continuous receptor stimulation, with pulse frequency and magnitude unchanged [4]; normalization of body weight and length in GHRH knockout mice under once-daily 2 µg subcutaneous administration for five weeks [8].
What the published clinical record has not measured: long-term body-composition outcomes in humans receiving CJC-1295, long-term safety, direct effects on testosterone or HPG-axis function (no direct effect demonstrated [3]), or efficacy in HIV-associated visceral obesity (the Phase 2 trial that would have produced that data was terminated [5][9]).
Reported Outcomes Across Studies
Reported Outcomes Across Studies
The Teichman 2006 Phase 1 study in healthy adults remains the principal human pharmacokinetic reference for CJC-1295-DAC: single ascending subcutaneous doses produced 2-10x mean GH elevation for six days or more and 1.5-3x mean IGF-1 elevation for nine to eleven days, with no serious adverse reactions reported at the tested doses [3]. The Ionescu 2006 study at 60 or 90 µg/kg subcutaneous reported a 7.5-fold trough GH elevation, 46% mean GH increase, 45% IGF-1 increase, and preserved pulsatile pattern [4].
The Alba 2006 preclinical study in GHRH knockout mice reported normalization of body weight and length under once-daily 2 µg dosing for five weeks, with reduced effectiveness when dosing was extended to 48- or 72-hour intervals — useful as a frequency-response reference even though the underlying pathology is not present in healthy human subjects [8].
No published Phase 2 or Phase 3 efficacy data exists. The 2006 Phase 2 lipodystrophy trial (NCT00267527) was terminated before completion and results were never posted [9].
The 2006 Terminated Phase 2 Trial
The 2006 Terminated Phase 2 Trial
ConjuChem opened a Phase 2 trial of CJC-1295 in HIV-associated visceral obesity in December 2005: NCT00267527, multicentre, randomized, placebo-controlled, N=192, with low-dose-escalation (60, 90, 120 µg/kg) and high-dose-escalation (60, 120, 240 µg/kg) arms once weekly [9]. On 17 July 2006 the trial was halted after a participant in Argentina died of a fatal myocardial infarction shortly after his 11th once-weekly dose [5]. The site investigator's attributed most likely cause was asymptomatic coronary artery disease with plaque rupture; the sponsor concluded the event was unlikely directly related to the peptide but discontinued industry development of CJC-1295 nonetheless [5]. Trial status on ClinicalTrials.gov is recorded as Terminated, with results not posted [9].
Context: independent of CJC-1295, GHRH-receptor agonists have shown cardioprotective effects in animal models of myocardial infarction — reduced infarct scar, improved ventricular remodeling — which is one reason the 2006 event was interpreted as most likely unrelated coronary disease rather than a class-level cardiotoxicity [11]. The trial halt nonetheless ended industry development, and no successor Phase 2 program has opened in the 19 years since.
CJC-1295 vs. Ipamorelin
CJC-1295 vs. Ipamorelin
CJC-1295 is a GHRH-receptor agonist. Ipamorelin is a selective ghrelin / GHS-R1a receptor agonist [12]. Different receptors, different signaling pathways, complementary GH-release mechanisms.
Ipamorelin's distinguishing pharmacological feature is selectivity: it releases GH with potency comparable to GHRP-6 but does not significantly elevate ACTH, cortisol, or prolactin even at doses 200-fold above its GH ED50 [12]. That selectivity is the rationale for pairing it with CJC-1295 in research protocols — CJC-1295 raises baseline GH release via the GHRH receptor while ipamorelin adds a pulsatile spike via the GHS-R1a receptor, and the two activations are receptor-distinct and additive [12].
CJC-1295 vs. ipamorelin: mechanism contrast
CJC-1295 is a GHRH analog acting on the GHRH receptor. Ipamorelin is a selective ghrelin/GHS-R1a receptor agonist [12]. Different receptors, complementary GH-release pathways. Co-administration in published provocation testing produces a supra-additive GH response larger than either alone [12].
Why CJC-1295 is paired with ipamorelin in research
The pair is studied as a complementary GH-stimulation strategy. CJC-1295 (GHRH analog) raises baseline GH release; ipamorelin (selective ghrelin mimetic) adds a pulsatile spike without affecting cortisol or prolactin [12]. The combined receptor activation is additive rather than redundant — distinct receptors, distinct signaling cascades, converging on GH release.
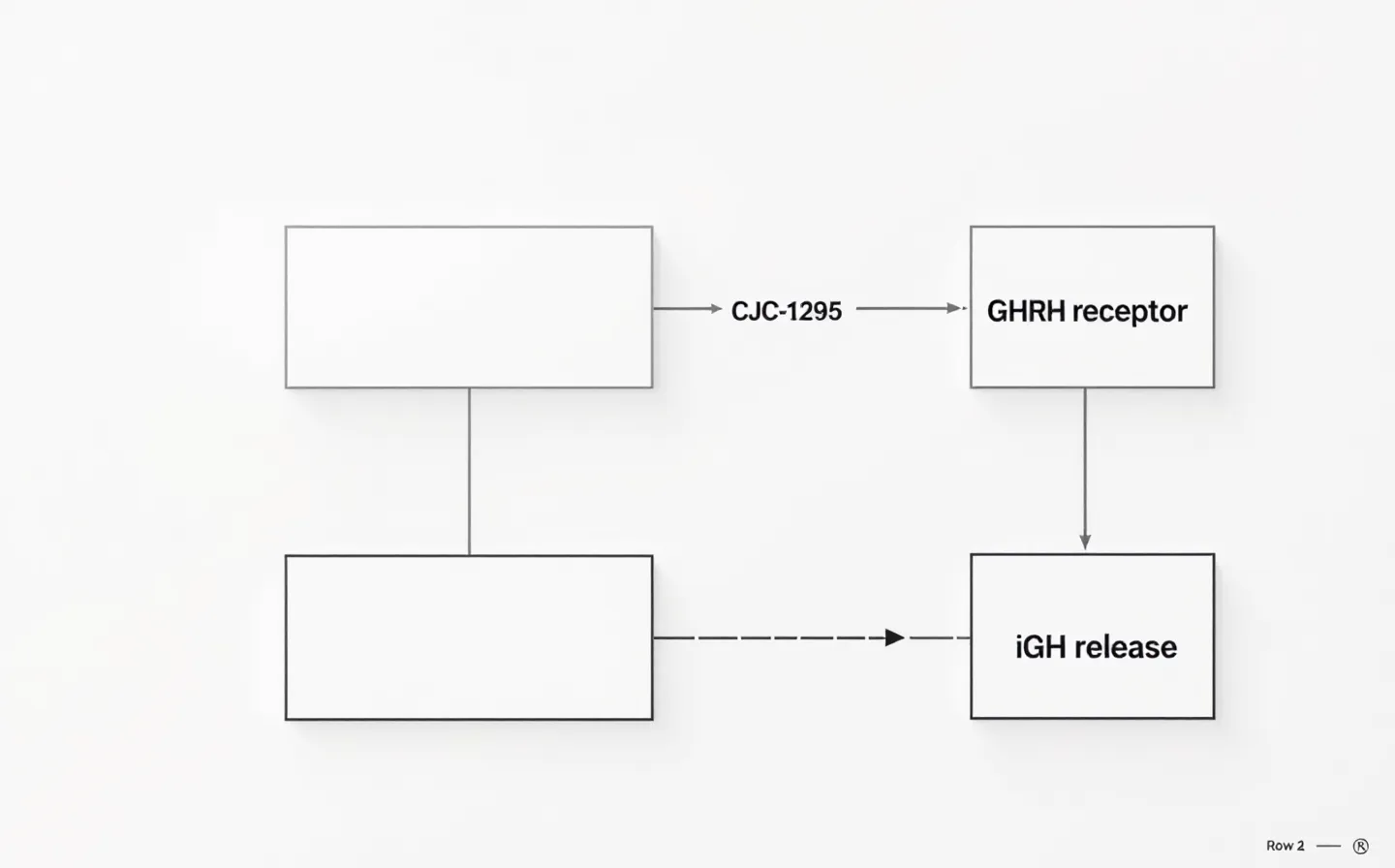
Fig. 03 / CJC-1295 vs. ipamorelin
GHRH-receptor pathway (top, cobalt-marked target) and GHS-receptor pathway (bottom) converging on GH release.
Time-course of measurable effects
Time-course of measurable effects
Pharmacological markers respond first. Serum GH elevates within hours of subcutaneous CJC-1295-DAC injection and remains elevated for six days or more after a single dose [3]. IGF-1 rises within the first 24-48 hours and remains elevated for nine to eleven days after a single dose; under weekly or biweekly dosing IGF-1 remains elevated for up to 28 days [3].
Body-composition outcomes have not been measured in completed human trials. The Phase 2 trial that would have produced those data was terminated before efficacy endpoints were reached [9]. User-reported timelines for subjective body-composition change typically describe 8-12 weeks of administration before perceptible effect, but this is observational and not validated against placebo control in published clinical research.